Snakebite Syndromes and Syndrome Management
in South African Snakebites
Progressive Weakness Syndrome
Neurotoxic Envenomation

Overview and Cause
The Progressive Weakness Syndrome is a critical, life-threatening manifestation of snake envenomation caused primarily by neurotoxic venoms. These venoms act on the nervous system, leading to muscle weakness and, ultimately, paralysis. In the South African context, this syndrome is most commonly associated with bites from Elapid snakes, including:
- Mambas: Black Mamba (Dendroaspis polylepis) and Green Mamba (Dendroaspis angusticeps).
- Non-Spitting Cobras: Cape Cobra (Naja nivea), Snouted Cobra (Naja annulifera), and Forest Cobra (Naja melanoleuca).
- Adders (less common but important): Berg Adder and Desert Mountain Adder.
The venom contains polypeptides that interfere with the transmission of signals between nerves and muscles (neuromuscular blockade). Mamba venoms, in particular, include toxins (dendrotoxins) that facilitate and then block the release of acetylcholine, while cobra venoms typically block the post-synaptic receptors, resulting in a paralysis that progresses to the diaphram and basically stops the victim breathing.
Clinical Features
The syndrome is characterized by a progressive, descending flaccid paralysis. Early symptoms often involve the muscles controlled by the cranial nerves, followed by paralysis of the trunk and limb muscles, and eventually, the muscles of respiration.
A memory aid for key signs can be used: 4 Ps and 4 Ss:
- Paralysis (general muscle weakness)
- Ptosis (drooping of the upper eyelids)
- Paraesthesia (numbness/tingling, often around the mouth and tongue)
- Pupillary dilatation (dilated pupils)
- Salivation (excessive drooling)
- Sweating (diaphoresis)
- Slurred speech (dysarthria)
- Swallowing difficulties (dysphagia)
Other features may include blurred or double vision, the “broken neck syndrome” (decreased neck muscle tone causing the head to slump forward), muscle spasms, and fasciculations (fine muscle twitching). The most feared complication is respiratory failure due to paralysis of the diaphragm and intercostal muscles, which can lead to cardiac arrest and death if not treated promptly.
Management
Management is focused on supportive care, early intubation/mechanical ventilation if paralysis progresses, and prompt administration of antivenom:
- Airway and Breathing: Continuous monitoring of respiratory function is crucial. Early intubation and mechanical ventilation are recommended for progressive paralysis. Ventilation may be required for several days, even after antivenom administration.
- Antivenom: The presence of any signs of neurotoxicity is a strong indication for the administration of the South African Institute of Medical Research (SAIMR) polyvalent antivenom.
- Pressure Immobilisation: Unlike cytotoxic bites, pressure immobilisation bandaging may be applied to the affected limb immediately after the bite and should only be removed once antivenom is ready to be administered in a controlled medical setting.
Bleeding Syndrome
Haemotoxic/Coagulopathic Envenomation

Overview and Cause
The Bleeding Syndrome, also known as coagulopathic or haemotoxic envenomation, is a systemic effect resulting from venoms that interfere with the blood clotting cascade. This is typically caused by the venoms of two specific back-fanged snakes in South Africa:
- Boomslang (Dispholidus typus)
- Vine Snake (Thelotornis capensis)
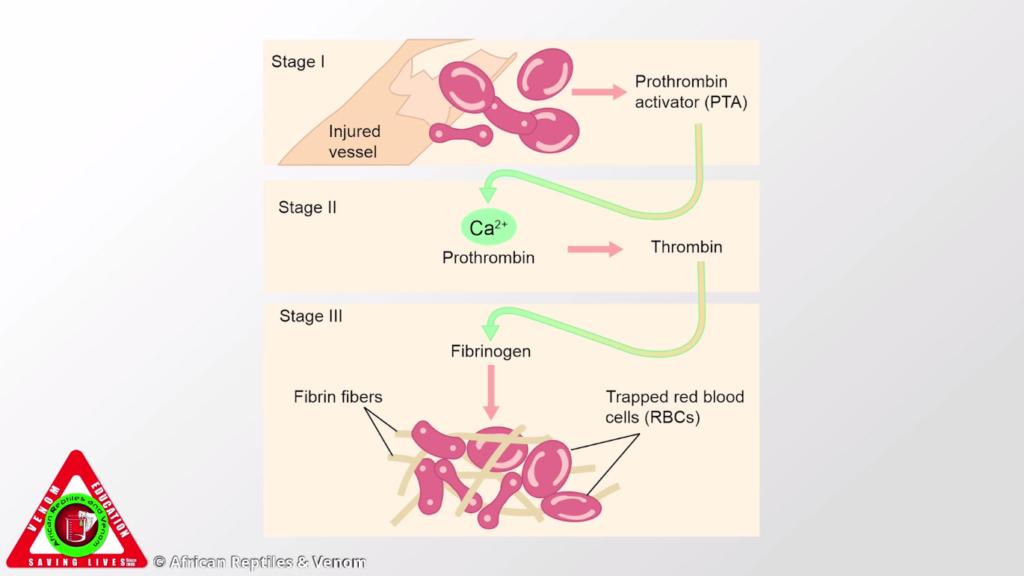
The venoms of these snakes are haemotoxic, specifically procoagulant toxins. They activate blood-clotting factors (like Prothrombin/Factor II and Factor X) leading to widespread, uncontrolled clotting inside the blood vessels (Venom-Induced Consumption Coagulopathy or VICC). This consumes all the available clotting factors (fibrinogen, platelets, etc.), resulting in a profound and delayed inability of the blood to clot.
Clinical Features
Crucially, early symptoms are often absent or minimal. The bleeding tendency develops over time, and the signs may be delayed, often appearing 12 to 36 hours post-bite.
- Early Signs (Delayed):
- Bleeding at the bite site or from old wounds/drip sites.
- Bruising (ecchymoses).
- Abnormal 20-minute Whole Blood Clotting Time (WBCT20) – often detectable within 30 to 60 minutes of the bite.
- Later/Severe Symptoms (Widespread Internal Bleeding):
- Bleeding from mucous membranes (gums, nosebleeds/epistaxis).
- Blood in the urine (haematuria) or stools (melena).
- Coughing up blood (haemoptysis).
- Cerebral haemorrhage (bleeding in the brain), which is the most common cause of death.
- Hypotension and hypovolaemic shock due to massive internal blood loss.
The clinical history may include the snake needing to be “pulled off” the bite site due to the chewing action associated with the back-fanged nature of these species.
Management
Management focuses on close observation, correction of the coagulopathy, and antivenom:
- Observation and Testing: A minimum 12-hour observation period is essential, with repeated checks of the WBCT20 (a simple bedside test) and formal clotting screens (INR, aPTT, Fibrinogen).
- Antivenom: Specific Monovalent Antivenom (Boomslang antivenom) is indicated. Note that the SAIMR polyvalent antivenom does not contain antibodies against Boomslang or Vine Snake venom.
- Blood Products: Correction of the coagulopathy with fresh frozen plasma (FFP) or cryoprecipitate may be required, in addition to antivenom.
Painful Progressive Swelling Syndrome
Cytotoxic Envenomation

Overview and Cause
The Painful Progressive Swelling (PPS) Syndrome is the most common form of serious snake envenomation seen in South Africa. It is caused by cytotoxic venoms which primarily cause local tissue damage. The main species responsible are:
- Adders: Puff Adder (Bitis arietans), Gaboon Adder (Bitis gabonica).
- Spitting Cobras: Mozambique Spitting Cobra (Naja mossambica), Black Spitting Cobra (Naja nigricollis).
- Other: Stiletto Snakes (Atractaspis spp.), Night Adders (Causus spp.).
Cytotoxic venoms cause cell death (necrosis) and increase the permeability of blood vessel walls (vascular endothelium). This leads to the rapid extravasation (leakage) of fluid, blood, and plasma from the vessels into the surrounding tissue, causing pain and massive swelling.
Clinical Features
This syndrome is characterized by rapid, severe local effects at the bite site:
- Local Symptoms:
- Immense pain at the bite site.
- Swelling (Oedema): Starting at the bite site and rapidly progressing up the limb, making the affected area warm and tense. Swelling progression is an indication of severity (e.g., swelling of the whole hand/foot within 1 hour, or up to the knee/elbow in less than 6 hours).
- Tissue Damage: Blistering (bullae), skin discoloration, and bleeding under the skin (subcutaneous haemorrhage/ecchymoses).
- Necrosis: Irreversible tissue death, which often develops over days and may require surgical debridement or skin grafting.
- Complications (Systemic and Regional):
- Hypovolaemic Shock: Internal organs like the kidneys, liver and heart struggle to operate properly due to massive fluid loss from the bloodstream into the swollen tissue, especially in children or if swelling is extensive.
- “Pseudo-compartment Syndrome”: The limb becomes extremely tense, mimicking true compartment syndrome. While true compartment syndrome is rare in snakebite, the pressure from the swelling can still compromise circulation and nerves.
- Acute Kidney Injury/Rhabdomyolysis: Less common, but can occur due to local muscle damage releasing broken-down muscle contents into the bloodstream.
Management
Management involves pain control, close monitoring, antivenom, and selective surgical review:
- Supportive Care and Analgesia: Pain relief (often requiring simple analgesia like paracetamol; NSAIDs and opiates are avoided due to complication risks).
- Antivenom: The SAIMR polyvalent antivenom is indicated for severe and progressively spreading cytotoxic envenomation (e.g., swelling progressing rapidly, or involving major joints/the trunk).
- Wound Care and Observation: The limb should be kept at the level of the heart (not excessively elevated). Blisters are typically left intact initially. Necrotic tissue should be allowed to demarcate (5-7 days) before conservative debridement.
- Compartment Syndrome: True compartment syndrome is rare, but the clinical suspicion of nerve and vessel compromise requires urgent surgical review. Fasciotomy (surgical release) should only be performed after careful diagnosis (ideally, measuring compartment pressures), as it is often an unnecessary and harmful procedure in cases of pseudo-compartment syndrome.
Complex and Unexpected Snakebite Syndromes (South African Context)
While the syndromic approach—categorizing bites as Neurotoxic, Cytotoxic, or Haemotoxic—is the gold standard for initial triage, several South African species present "mixed" clinical pictures or symptoms that defy their family’s typical venom profile.
1. Species with Combined or Unexpected Syndromes
Snouted Cobra (Naja annulifera)
- The Syndrome Mix: Historically considered purely neurotoxic, the Snouted Cobra is now recognized for a potent dual-syndrome
- Clinical Presentation: Victims typically develop Progressive Weakness Syndrome (neurotoxicity) alongside significant Painful Progressive Swelling (cytotoxicity).
- Key Detail: Unlike the Cape Cobra (Naja nivea), which causes minimal local reaction, Snouted Cobra bites frequently lead to localized tissue necrosis. This sometimes requires surgical debridement or skin grafting even after the neurotoxic symptoms have been stabilized with antivenom.
Green Mamba (Dendroaspis angusticeps)
- Unexpected Cytotoxicity: While the Black Mamba ( polylepis) is famous for its “clean” bite (massive neurotoxicity with almost no swelling), the Green Mamba frequently causes marked local oedema and pain.
- Diagnostic Trap: The presence of swelling can occasionally mislead first responders into diagnosing a purely cytotoxic bite (like an Adder), potentially delaying the administration of polyvalent antivenom or respiratory support required for the inevitable neurotoxic progression.
Berg Adder (Bitis atropos)
- The Anomalous Adder: Most adders in South Africa are purely cytotoxic. The Berg Adder is a significant exception, possessing a complex venom that is primarily neurotoxic, specifically targeting the cranial nerves.
- Unique Symptoms: It causes a unique syndrome including loss of smell (anosmia), loss of taste, and ophthalmoplegia (paralysis of the eye muscles leading to fixed, dilated pupils). These symptoms can persist for weeks or even months. Notably, the SAIMR Polyvalent Antivenom is ineffective against Berg Adder venom.
Rinkhals (Hemachatus haemachatus)
- The Cytotoxic Elapid: Though it is an elapid (related to cobras), the Rinkhals presents almost exclusively with Painful Progressive Swelling.
- Clinical Picture: Serious neurotoxicity (respiratory failure) is clinically rare in human Rinkhals bites; the primary concern is usually local tissue destruction and necrosis at the bite site.
2. The Use of Neostigmine in Snouted Cobra Bites
Neostigmine is an acetylcholinesterase inhibitor that can serve as a life-saving adjunctive therapy in specific neurotoxic envenomations, particularly those involving cobras.
Mechanism of Action
- Post-Synaptic Blockade: Cobra venoms (including the Snouted Cobra) contain α-neurotoxins that bind to nicotinic acetylcholine receptors at the neuromuscular junction. This blocks the signal from the nerve to the muscle.
- How Neostigmine Works: It prevents the breakdown of acetylcholine, increasing its concentration at the neuromuscular junction. This excess acetylcholine “competes” with the venom for the receptors, potentially reversing the paralysis.
Application Protocol
- The Atropine Challenge: Before administering Neostigmine, Atropine must be given intravenously to block the muscarinic side effects of Neostigmine (such as bradycardia, excessive salivation, and bronchial secretions).
- Trial Dose: A trial dose of Neostigmine is administered. If the patient shows visible improvement (e.g., an increase in the ability to lift eyelids or improved respiratory effort), a continuous infusion or regular bolus may be maintained.
- Bridge to Recovery: Neostigmine is not a replacement for antivenom. It is a supportive measure to buy time and potentially reduce the duration of mechanical ventilation while the antivenom (or the body’s natural metabolism) clears the toxins.
Critical Limitation: The “Mamba Rule”
- Ineffectiveness: Neostigmine is ineffective against Mamba envenomation.
- Reason: Mamba venoms contain dendrotoxins that act pre-synaptically (affecting the release of acetylcholine from the nerve end) rather than blocking the receptors. Since the receptors aren’t blocked, increasing acetylcholine via Neostigmine provides no therapeutic benefit and may exacerbate symptoms.



